
Adrenal Fatigue? Adrenal Insufficiency? Cortisol? PseudoCushing’s Syndrome? What do these terms mean and why are they all over the internet these days? And, what do they have to do with your weight loss?
This was our topic this evening on PeriScope. Katch Dr. Nally speak about this topic with rolling comments at Katch.me/docmuscles. Or you can watch the video below:
If you’re not sure about what this is, you’re not alone. I think I’ve heard the term “Adrenal Fatigue” at lease four times a day for the last three months. If you ask your doctor, they’ll probably scratch their heads too. The funny thing is that “Adrenal Fatigue” isn’t a real diagnosis, but it is all over the internet and it shows up in the titles of magazines in the grocery store every day. There’s even and “Adrenal Fatigue For Dummies” so it must be real, right?! 
No. It isn’t a real diagnosis. It is a conglomeration of symptoms including fatigue, difficulty getting out of bed in the morning, and “brain fog” that have been lumped together to sell an “adrenal supplement.” (Sorry, but that’s really what it is all about.) Do a Google search and the first five or six sites describing adrenal fatigue claim the solution is taking their “special adrenal supplement.”
I know what you’re thinking, “Your just a main stream, Western Medicine doctor, Dr. Nally, you wouldn’t understand.” Actually, I do understand.
Adrenal fatigue has risen in popularity as a “lay diagnosis” because many patients show up at their doctors office with significant symptoms that actually interfere with their ability to function, and after all the testing comes back negative for any significant illness, they are told that they are normal. But the patient still has the symptoms and no answer or treatment has been offered. It’s discouraging. . . very discouraging.
That’s because the symptoms are actually the body’s response to chronic long term stress. Many of my patients, myself included, have found themselves “stuck” in their weight loss progression, feeling fatigued, struggling to face the day, with a number of symptoms including cold intolerance, memory decline, difficulty concentrating, depression, anxiety, dry skin, hair loss, and even infertility in some cases. Is it poor functioning adrenal glands? No, your feeling this way because the adrenal glands are actually doing their job!!
If the adrenal glands weren’t working you’d experience darkening of the skin, weight loss, gastric distress, significant weakness, anorexia, low blood pressure, and low blood sugar. The symptoms are actually called Addison’s disease and it is actually fairly rare (1 in 100,000 chance to be exact). So what is causing the symptoms you ask?
There are a number of reasons, but one that I am seeing more and more frequently is “Pseudo-Cushings’s Syndrome.” Pseudo-Cushing’s Syndrome is a physiologic hypercortisolism (over production of cortisol) that can be caused by five common issues:
- Chronic Physical Stress
- Severe Bacterial or Fungal Infections that Go Untreated
- Malnutrition or Intense Chronic Exercise
- Psychological Stress – including untreated or under-treated depression, anxiety, post-traumatic stress, or dysthymia (chronic melancholy)
- Alcoholism
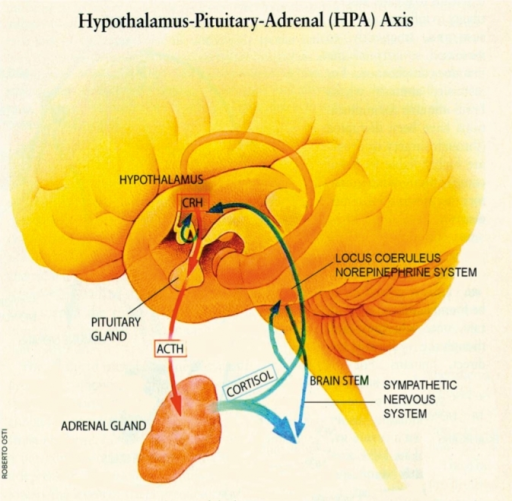
The psychiatric literature suggest that up to 80% of people with depressive disorders have increased cortisol secretion (1,2,3).  People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true Cushing’s Syndrome, but has the effect of the symptoms listed above and begins with limiting ones ability to loose weight.
People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true Cushing’s Syndrome, but has the effect of the symptoms listed above and begins with limiting ones ability to loose weight.
I’m convinced that this is becoming more and more prevalent due to the high paced, high-stress, always on, plugged in, 24 hour information overload lives we live.
What is cortisol? It is a steroid hormone made naturally in the body by the adrenal cortex (outer portion of the adrenal gland). Cortisol is normally stimulated by a number of daily activities including fasting, awakening from sleep, exercise, and normal stresses upon the body. Cortisol release into the blood stream is highest in the morning, helping to wake us up, and tapers into the afternoon. Cortisol plays a very important role in helping our bodies to regulate the correct type (carbohydrate, fat, or protein) and amount of fuel to meet the bodies physiologic demands that are placed upon it at a given time (4,5,6).
 Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
aches, hypertension, depression, anxiety, hair loss, dry skin and ankle edema, to name a few.
The chronic elevation in cortisol directly stimulates increased insulin formation by increasing the production of glucose in the body, and cortisol actually blunts or block-aids the thyroid function axis. Both of these actions halt the ability to loose weight, and drive weight gain.
Cortisol also increases appetite (10). That’s why many people get significant food cravings when they are under stress (“stress eaters”). Cortisol also indirectly affects the other neuro-hormones of the brain including CRH (corticotrophin releasing hormone), leptin, and neuropeptide Y (NPY). High levels of NPY and CRH and reduced levels of leptin have also been shown to stimulate appetite and cause weight gain (10-11).
How do you test for Pseudo-Cushing’s Syndrome?
Testing can be done by your doctor with a simple morning blood test for cortisol. If your cortisol is found to be elevated, it needs to be repeated with an additional 24 hour urine cortisol measurement to confirm the diagnosis. If Cushing’s Syndrome is suspected, some additional blood testing and diagnostic imaging will be necessary. Pseudo-Cushing syndrome will demonstrate a slightly elevated morning cortisol that doesn’t meet the criteria for true Cushing’s type syndrome or disease.
How do you treat it?
First, the stressor must be identified and removed. Are you getting enough sleep? Is there an underlying infection? Is there untreated anxiety or depression present? Are you over-exercising? These things must be addressed.
Second, underlying depression or anxiety can be treated with counseling, a variety of weight neutral anti-depressant medications or a combination of both. Many of my patients find that meditation, prayer, and journaling are tremendous helps to overcoming much of the anxiety and depression they experience.
Third, adequate sleep is essential. Remove the television, computer, cell phone, iPad or other electronic distraction from the bedroom. Go to bed at the same time and get up at the same time each day. Give yourself time each day away from being plugged in, logged in or on-line.
Fourth, mild intensity (40% of your maximal exertion level) exercise 2-3 days a week was found to lower cortisol; however, moderate intensity (60% of your maximal exertion level) to high intensity (80% of your maximal exertion level) exercise was found to raise it (12). A simple 20 minute walk, 2-3 times per week is very effective. Find a hobby that you enjoy and participate in it once or twice a week. Preferably, a hobby that requires some physical activity. The activity will actually help the sleep wake cycles to improve.
Fifth, follow a low carbohydrate or ketogenic diet. Ketogenic diets decrease insulin and reverse the effect of long term cortisol production. Ketogenic diets a have also been shown to decrease or mitigate inflammation by reducing hyperinsulinemia commonly present in these patients (13).
So, the take home message is . . . take your adrenal glands off of overdrive.
References:
- Pfohl B, Sherman B, Schlechte J, Winokur G. Differences in plasma ACTH and cortisol between depressed patients and normal controls. Biol Psychiatry 1985; 20:1055.
- Pfohl B, Sherman B, Schlechte J, Stone R. Pituitary-adrenal axis rhythm disturbances in psychiatric depression. Arch Gen Psychiatry 1985; 42:897.
- Gold PW, Loriaux DL, Roy A, et al. Responses to corticotropin-releasing hormone in the hypercortisolism of depression and Cushing’s disease. Pathophysiologic and diagnostic implications. N Engl J Med 1986; 314:1329.
- Ely, D.L. Organization of cardiovascular and neurohumoral responses to stress: implications for health and disease. Annals of the New York Academy of Sciences (Reprinted from Stress) 771:594-608, 1995.
- McEwen, B.S. The brain as a target of endocrine hormones. In Neuroendocrinology. Krieger and Hughs, Eds.: 33-42. Sinauer Association, Inc., Massachusetts, 1980.
- Vicennati, V., L. Ceroni, L. Gagliardi, et al. Response of the hypothalamic- pituitary-adrenocortical axis to high-protein/fat and high carbohydrate meals in women with different obesity phenotypes. The Journal of Clinical Endocrinology and Metabolism 87(8) 3984-3988, 2002.
- Wallerius, S., R. Rosmond, T. Ljung, et al. Rise in morning saliva cortisol is associated with abdominal obesity in men: a preliminary report. Journal of Endocrinology Investigation 26: 616-619, 2003.
- Epel, E.S., B. McEwen, T. Seeman, et al. Stress and body shape: stress-induced cortisol secretion is consistently greater among women with central fat.
Psychosomatic Medicine 62:623-632, 2000. - Tomlinson, J.W. & P.M. Stewart. The functional consequences of 11_- hydroxysteroid dehydrogenase expression in adipose tissue. Hormone and Metabolism Research 34: 746-751, 2002.
- Epel, E., R. Lapidus, B. McEwen, et al. Stress may add bite to appetite in women: a laboratory study of stress-induced cortisol and eating behavior.Psychoneuroendocrinology 26: 37-49, 2001.
- Cavagnini, F., M. Croci, P. Putignano, et al. Glucocorticoids and neuroendocrine function. International Journal of Obesity 24: S77-S79, 2000.
- Hill EE, Zack E, Battaglini C, Viru M, Vuru A, Hackney AC. Exercise and circulating cortisol levels: the intensity threshold effect. J Endocrinol Invest. 2008. Jul;31(7):587-91.
- Fishel MA et al., Hyperinsulinemia Provokes Synchronous Increases in Central Inflammation and β-Amyloid in Normal Adults. Arch Neurol. 2005;62(10):1539-1544. doi:10.1001/archneur.62.10.noc50112.
 People with significant stressors in their life have been show to have a raised cortisol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing an over production of cortisol and normalization of their cortisol levels occurs after resolution of the stressor. This cortisol response is not high enough to lead to a true
People with significant stressors in their life have been show to have a raised cortisol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing an over production of cortisol and normalization of their cortisol levels occurs after resolution of the stressor. This cortisol response is not high enough to lead to a true 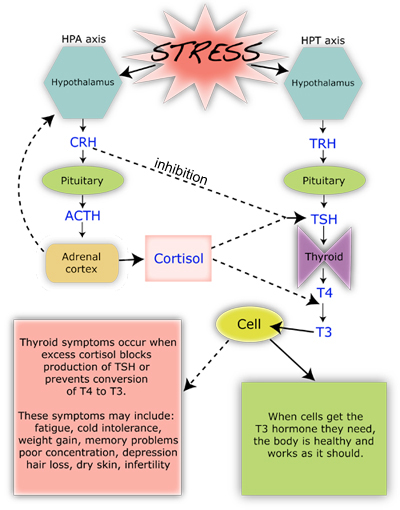 Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues and turns on the maturation process of adipocytes (fat cells). In the process, it suppresses the immune system to decrease inflammation during times of stress (7,8,9). In the short run, this is an important process, however, when cortisol production is chronically turned up, it leads to abnormal deposition of fat, increased risk of infection, impotence, abnormal blood sugars, head
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues and turns on the maturation process of adipocytes (fat cells). In the process, it suppresses the immune system to decrease inflammation during times of stress (7,8,9). In the short run, this is an important process, however, when cortisol production is chronically turned up, it leads to abnormal deposition of fat, increased risk of infection, impotence, abnormal blood sugars, head